Be aware that patients now are more informed and may have a Do Not Attempt Resusitation order (DNAR). Many times EMS is called to help family deal with the dying process and resusitation should not be attempted. This is an end of life issue, not a life saving issue.
If this is not the case, proceed:
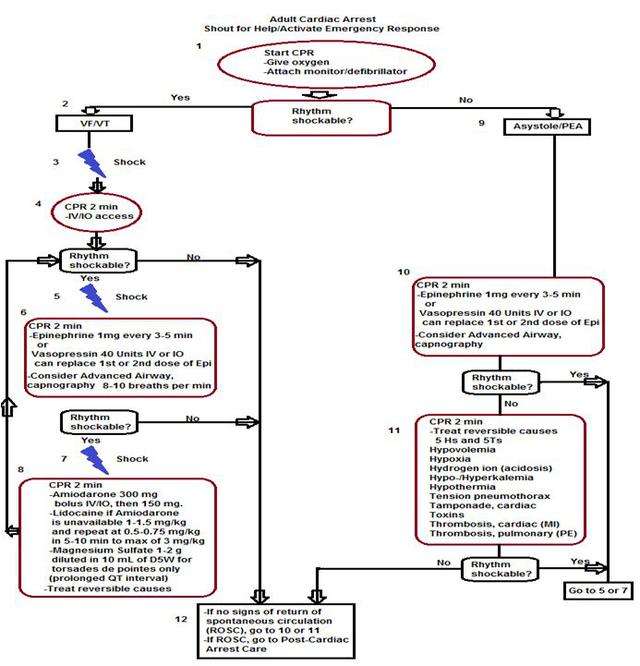
*Person Collapses (Adult, assume cardiac arrest)
*Check Responsiveness and Breathing - simultaneously (Tap and Shout) "Are you okay?" - If unresponsive or if pt is not breathing or is agonally breathing, then
*Call emergency response system (call 911 or if in a medical setting call a code blue or retrieve a
defibrillator/AED if available) - the main rhythm associated with cardiac arrest in an adult is V.fib or
Pulseless V. Tach and NEEDS to be shocked as soon as possible to survive.
Begin BLS - Primary Assessment:
C-CIRCULATION (3 steps):
1. Check responsiveness and for breathing – Tap and shout, "Are you okay?”
Check responsiveness and for breathing – Tap and shout, "Are you okay?”
– look for chest rise – if no response or breathing or
abnormal breathing go to next step
2.Call a Code Blue if in hospital or if out of hospital Call 9-1-1
3.a. Check Circulation- by palpating a carotid/femoral pulse (within 10
seconds). If no definite pulse within 10 seconds then, begin chest
compressions. If a definite pulse is felt, then give 1 breath every 6
seconds for adults and 1 breath every 2-3 seconds for children and
infants. Recheck pulse every 2 minutes or 5 cycles.
b. Provide - CIRCULATION w/chest compressions and ventilations
(30:2) for at least 100-120 compressions per minute, “hard and fast”, at
least 2 inches deep with minimal interruptions. Allow for complete
recoil of the chest after each compression.
A-AIRWAY: Open the AIRWAY using head-tilt-chin lift, if trauma suspected, then use jaw thrust method. Even if trauma suspected and you are the only rescuer available, then open the airway using head-tilt-chin lift.
B- BREATHING: Assessment of this was done in step one - Provide BREATHING (2 breaths) allowing the chest to rise each time, give each breath over 1 second. Avoid excessive ventilations. If the breath does not go in, reposition the head by head-tilt-chin lift and attempt to deliver 2 breaths. Utilizing a bag-valve-mask (BVM) requires a good seal – E-C method, E with 3 fingers along jawbone and C with thumb and forefinger on the mask. Please note that this is best done with 2 rescuers and not recommended for the single lone rescuer.
Helps arrives and begins D for defibrillation, or if patient has a definite pulse, then skip to the secondary survey.
D=Defibrillation, Attach to a defibrillator-monitor or with paddles do a quick look for a shockable rhythm. We are looking for V.fib or V.Tach to defibrillate.
Secondary Assessment:
C=Circulation: Resume CPR with Chest Compressions 30:2; Start IV preferred route and in the antecubital space or IO (Intraosseous if peripheral unable to be obtained), Give meds
A=Airway - Is the airway open and patent? If not, secure the an airway with an advanced airway device. Intubate patient with an ET tube or another
advanced airway (see below for different types and for a discussion on
intubation). Continuous waveform capnography is recommended as
the recommended secondary confirming technique and recommended
for maintaining correct placement of the endotracheal tube. Class I.
PETCO2 (partial pressure of end tidal carbon dioxide) normal range is 35-40 mmHg. If < 10 mmHg, in arrest, then improve the quality of
CPR.
B=Breathing - Are ventilation and oxygenation adequate? Place on oxygen and/or confirm placement with capnography. Once the advanced airway is in place. RR then should be 1 breath every 6 seconds (10 breaths per min) and NOT syncronized with chest compressions. If patient has a pulse and does NOT have an advanced airway, then ratio is 1 breath every 6 seconds. .
D=Determine the cause - look for 5 Hs and 5 Ts: Hypovolemia, Hypoxia, Hydrogen Ion (Acidosis), Hypo/hyperkalemia (low or high K level), Hypothermia, & Tension Pneumothorax, Tamponade-cardiac, Toxins (overdose - see PEA for tx), Thrombosis-pulmonary (Pulmonary Embolism-PE), Thrombosis-cardiac (Myocardial Infarction-MI).
**Confirm asystole in a second lead and make sure all your leads are attached to the patient and the monitor. This is done to check for a fine V.Fib in another lead and to treat the patient, not the monitor if a lead is loose or disconnected.**
Give:
Epinephrine 1 mg IV q 3-5 minutes
Vasopressin has been eliminated in PEA and Asystole algorithms for 2015.
Flush with 20mL NS or run IVFs to keep meds running into the vein and raise the arm. After giving the drug, then resume CPR for 30 - 60 seconds to help circulate the medication, remember the only heartbeat is the one your manually give the patient.
D=Differential Diagnosis, Search for and treat reversible causes including but not limited to 5 Hs and 5 Ts:
Hypovolemia-give fluids and/or blood products (the #1 cause of PEA),
Hypoxia-give 100% ventilated oxygen,
Hypo/hyperkalemia(low or high K level)-give KCL boluses for low K+ level/-give NaHCO3 1mEq/kg IV q 10 minutes for high K+ level,
Hydrogen Ion (acidosis)-hyperventilate pt or give NaHCO3 depending upon lab values,
Hypothermia - warmed IVFs for hypothermia,
Thrombosis Pulmonary (PE)-thrombolytics or surgery to remove the blockage,Thrombosis Cardiac (MI)-thrombolytics or surgery to remove the blockage, Tension Pneumothorax-needle decompression,
Cardiac Tamponade-paracardial centesis,
Toxins - Used to be called Tablets (OD)-give NaHCO3 for certain antidepressants. See PEA (at bottom) for Opiod Associated Life Threatening Emergency Algorithm - New 2015.
See PEA algorithm for a detailed explanation of each.
Consider terminating efforts